تتمثل التفاوتات الصحية (وجود اختلافات غير عادلة، أو قابلة للتجنب، أو قابلة للتصحيح في تحقيق الصحة والرفاهية الأمثل بين الناس) في تحديات مستمرة وعاجلة على الصعيدين العالمي والمحلي [تانغتشارونساثيان، 2023]. هناك بعض المجموعات السكانية التي تتأثر بشكل غير متناسب ببعض الأمراض، وتتحمل عبءًا أكبر من سوء الصحة، ولديها وصول أقل إلى خدمات الصحة الجيدة، وتختبر متوسطات أعمار أقصر. تعتمد عملية تقليل التفاوتات الصحية بشكل كبير على الجهود المبذولة نحو الوصول إلى التغطية الصحية الشاملة والهدف الثالث من أهداف التنمية المستدامة (SDG 3.8)، والذي يسعى لضمان حصول جميع الأشخاص، بغض النظر عن ظروفهم، على الرعاية الصحية الجيدة دون مواجهة خطر الإفقار المالي. تجذر التفاوتات الصحية عميقاً ومتشابكة بين العوامل التاريخية، والهيكلية، والاجتماعية، والاقتصادية، والبيئية. ونتيجةً لذلك، كلاً من البحث في التفاوتات الصحية والإجراءات السياسية لتقليلها معقد ومتنوع، ويتطلب جهودًا متعددة القطاعات وشمولية.
This research axis is coordinated by Joana Orne Gliemann (UB) and Chishala Chabala (UNZA),
Overall motivation
Health inequities (presence of unfair, avoidable or remediable differences in achieving optimal health and well-being among people) are persistent and urgent challenges globally and locally [Tangcharoensathien, 2023]. Certain population groups are disproportionately affected by some diseases, bear a greater burden of ill-health, have less access to quality health services and experience shorter life expectancies. Reducing health inequalities highly depends on the efforts made towards reaching universal health coverage and Sustainable Development Goal (SDG) 3.8, which seeks to ensure that all people, whatever their circumstances, have access to quality healthcare without facing the risk of financial impoverishment. The roots of health inequalities are deep and entangled between historical, structural, social, economic and environmental factors. Consequently, both research into health inequalities and the policy actions to reduce them are complex and diverse, and require holistic multisectoral effort.
The objective of this axis is to conduct interdisciplinary research on Global Health inequities and poverty related diseases (PRDs), including through large-scale intervention studies and contribute to the transfer into policies of the research findings and the comprehensive, complex, multifactorial evidence-based interventions assessed.
Integrated activities
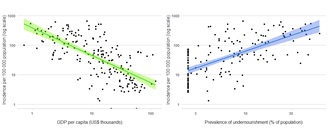
- Tuberculosis: This leading global infectious disease killer is typically a disease of poverty, reflecting both inequalities at individual and country level. According to the World Health Organization (WHO), there is a clear linear correlation between TB incidence at country level and the gross domestic product (GDP) per capita as well as the prevalence of undernourishment in the population (Figure). Within countries, at individual level, being poor increases the risk of falling sick with tuberculosis. Tuberculosis is associated with catastrophic costs incurred by families which further challenges access to care and worsens poverty.
- Under-five mortality: The probability that a newborn would die before reaching five years of age, expressed per 1,000 live births, is also both a global health indicator and a key indicator of poverty. In 2020, worldwide, under-five mortality ranged from 4 to 151 per 1,000 live births in children born in the poorest households, while it ranged from 2 to 96 in the richest [UNICEF, 2023]. Furthermore, the major causes of under-five mortality are what are called “poverty-related diseases” (PRDs) that encompass HIV-infection, tuberculosis, malaria, but also diarrheal infections and lower respiratory infections, all highly associated with contexts of undernutrition. These diseases are very much linked to the debilitating conditions of poverty, such as a lack of access to proper sanitation, health education and safe drinking-water, indoor air pollution due to biomass combustion, and malnutrition.
- Severe acute malnutrition (SAM): This most severe form of malnutrition, affects over 13 million children <5 years old worldwide. It encompasses both severe wasting and edematous malnutrition (kwashiorkor). These conditions are embedded in contexts of high poverty, constrained food systems, population displacements, catastrophic consequences of climate change. SAM is a major risk factor for death due to pneumonia and diarrhea in children<5 years and it increases the risk of developing tuberculosis, of being undiagnosed for the disease, and for having worse treatment outcomes including death compared to well-nourished children [Vonasek, 2022]. SAM is therefore both a marker and a disease of poverty.
Academic validation
The achievements of the GHI axis during the 1st cycle of IPORA funding include co-publishing 11 articles releasing the results of key projects funded prior to IPORA but which benefited from IPORA interdisciplinary networking during analysis, carrying out 1 IPORA-funded seed projects, preparing and obtaining external funding for 4 new projects, and initiating 4 PhDs. The work of this research axis contributed to the emergence of a new IRD-funded project named JEAI SPADE-KZ (Strengthening the fight against Poverty related DiseasEs in children (Kids). JEAI SPADE-KZ aims to strengthen the capacities of the University of Zambia (UNZA) Paediatric HIV and TB clinical research unit in the field of public health, epidemiology, social sciences, health economics. As a global health research team, with a strong paediatric clinical expertise, the UNZA Paediatric HIV and TB clinical research unit will have sustainable capacity to conduct interdisciplinary research on PRDs in children, in partnership with the GHiGS/UB team, the Ministry of Health / National Tuberculosis and Leprosy Program and other line ministries that play a key role in the transfer of health interventions and research results into policy and practice. This will prepare for future large-scale intervention studies to address under-five mortality and poverty-related diseases in Zambia, and the southern African region.





