This research axis is coordinated by Véronique Yoboue (UFHB) and Olivier Marcy (UB)
Overall motivation
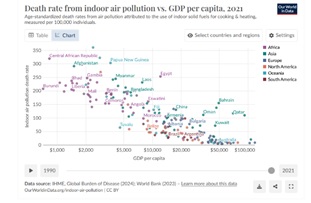
Populations from LMIC are largely exposed to air pollution, particularly household pollution caused by the use of low-cost, accessible biomass fuels for cooking and heating, with a clear relationship between GDP per capita and deaths from indoor air pollution (see side Figure). By 2019, almost 3 billion people were using biomass fuels such as wood, coal, animal dung, agricultural residues and oil to cook, heat and light their homes. In 2019, only 19% of the population in the African region had access to clean energy, compared to 90% in the European and American regions. The use of biomass fuels in poorly ventilated homes, combined with inefficient cooking methods, exposes people to Particulate Matter (PM) concentrations that are sometimes 100 times higher than the thresholds recommended by the WHO.
Despite the hight burden of non-communicable and communicable diseases due to air pollution, these are rarely considered as public health priorities in LMICs, still facing the heavy burden of pandemic infectious diseases such as HIV, malaria, and tuberculosis. Pollution legislation is weak or unenforced. For most countries in sub-Saharan Africa, there is a lack of ambient air quality monitoring, combined with insufficient capacity to collect population health data, which are major barriers to evidence-based intervention research on the subject. Within LMICs, the poorest populations are more exposed to pollution and are also the populations with the least knowledge on air pollution. Innovative approaches are needed to reduce use of biomass combustion or its impact on health. Such innovations may include electric cooking or improved cookstoves but there is still a lack of research data for their potential adoption.
Integrated activities
Two founding members of IPORA from two different disciplines and two different countries found a complementary interest and skills to capitalize on their expertise, join forces to tackle new issues and involve new partners in their thinking. The LASMES (LAboratoire des Sciences de la Matière, de l‘Environnement et de l’énergie Solaire) team in UFHB, Abidjan, had a history of research on domestic pollution, but this research did not have a health component targeted on children, a highly vulnerable population in front of air pollution. The GhiGS team in UB, France, had a history of research on respiratory pathology in young children, particularly in the field of tuberculosis. The two teams came together to set up a research agenda on the consequences of domestic pollution on child health, and integrated clinical research teams, economists, community members and ministerial authorities into their work.
This agenda includes research on the impact of pollution on respiratory health in children and their family entourage, and on large-scale complex interventions to mitigate domestic air pollution and its health impact.
Academic validation
The achievements of this research axis during the 1st cycle of IPORA funding include: publishing or presenting at conference 9 articles releasing the results of IPORA seed project or key projects funded prior to IPORA but benefited from IPORA interdisciplinary networking during analysis; preparing/carrying out 4 IPORA-funded seed projects; preparing 2 projects (Airyouth and electric cooking) that involve 4 new partners (Groningen Research Institute on Asthma and COPD [GRIAC], Netherlands; Bayreuth University, Germany; University of Bratislava, Slovakia; Université des Antilles, France); obtaining external funding for 1 new project (electric cooking); and initiating 1 PhD. The work of this research axis contributed to the emergence of a new IRD-funded network named REALLITYS. REALLITYS associates 9 French research teams, including GHiGS at UB, and 13 partner Institutions in 5 African countries, including UFHB in Côte d’Ivoire, to study the relationship between respiratory health and air quality in large African cities, in order to provide insights and policy-oriented recommendations for improving air quality and reducing its health impact on populations, whilst simultaneously participating in the development of sustainable cities. Disciplines of the teams involve: epidemiology, clinical medicine, ecology, pneumology, atmospheric chemistry and physics (ACP), modeling, demography, geography, climate, remote sensing, sociology, and immunology.





