The End TB Strategy adopted by the World Health Assembly in 2014 aims to end the global tuberculosis (TB) epidemic by 2035 and to reduce TB deaths by 95%. The operationalisation of this strategy calls for innovative approaches and health technologies for TB prevention and care in the most vulnerable and most affected populations. Furthermore, bringing together researchers, end-users, decision-makers and program implementers is crucial to shorten time between the generation of scientific evidence and widespread adoption of policies and improved practices for childhood TB, that can contribute to reaching the Sustainable Development Goals (SDGs).
- Summary :
- Background and rationale:
The End TB Strategy adopted by the World Health Assembly in 2014 aims to end the global tuberculosis (TB) epidemic by 2035 and to reduce TB deaths by 95%. The operationalisation of this strategy calls for innovative approaches and health technologies for TB prevention and care in the most vulnerable and most affected populations. Furthermore, bringing together researchers, end-users, decision-makers and program implementers is crucial to shorten time between the generation of scientific evidence and widespread adoption of policies and improved practices for childhood TB, that can contribute to reaching the Sustainable Development Goals (SDGs).
Each year an estimated 1.2 million children and young adolescents (<15 years) develop TB [2], of which more than 50% are aged below 5 years [3]. Modelling suggests that nearly 250,000 children die from TB yearly, and that over 95% of those dying of TB are undiagnosed. Globally, only 44% of children with TB are notified to the World Health Organization (WHO) by National TB Programs (NTPs), mainly because they are not diagnosed and consequently not treated. In children below 5 years this figure is as low as 35%. Low case detection is largely due to the paucibacillary nature of the disease and challenges in respiratory sample collection contributing to the low microbiological yield in children. Once diagnosed and treated, outcomes for children with TB are generally excellent with <1% mortality, but the case fatality rate for untreated TB can reach 44% in children below 5 years [6]. Children with inadequate immunity [e.g. children living with HIV (CLHIV), or those with severe acute malnutrition (SAM)] or severe pneumonia are at higher risk of underdiagnosis and of dying from TB.
WHO has identified that improvement in TB diagnostics is the highest research priority in the field of child TB. Currently, in the absence of highly sensitive TB diagnostic tool for children, most children are started on treatment only on the basis of high clinical suspicion. Treatment decision algorithms (TDAs), that assign scores to clinical and radiographic features or microbiological tests and recommend TB treatment initiation above a pre-defined total score, can enable rapid and uniform treatment decision-making. In March 2022, WHO issued an interim and conditional overall recommendation to use TDAs to diagnose pulmonary TB in children below 10 years. Furthermore, in the accompanying operational handbook [12], WHO suggested two specific TDAs for use in settings with and without access to chest X-ray (CXR), with a single diagnostic approach in both the general paediatric population and high-risk groups (age <2, CLHIV, and SAM). WHO has stated that external validation of these algorithms is an urgent priority in view of the conditional recommendation[1].
Decentralizing childhood TB services is essential to increase access to TB diagnosis. Use of TDAs at lower levels of care by overburdened Health Care Workers (HCWs) with limited child TB experience will require strengthening clinical skills and treatment decision-making capacity. Data on the diagnostic accuracy of TDAs, their feasibility, acceptability by end-users, effectiveness, and cost-effectiveness are crucial to update the current WHO policy and operational handbook, national policies, and clinical curricula. A comprehensive TB TDA-based approach could integrate other specific TDAs developed for CLHIV and those with SAM if they outperform the WHO-suggested TDAs and would also provide the opportunity to integrate a disease severity assessment step to assess eligibility for a shorter (4-month) treatment for non-severe TB cases in children as recommended by the WHO. Importantly, tools for integrated TDAs should be tailored to the needs and existing clinical practices of HCWs at primary health centre (PHC) and district hospital (DH) level, to which innovative digital tools (such as clinical decision support systems – CDSS) could contribute, in order to enhance adoption, delivery, and quality of decentralized TB services.
- Objectives :
General : to generate scientific evidence for the implementation of a comprehensive Treatment Decision Algorithm (TDA)-based approach for screening, diagnosis and management of tuberculosis (TB) in children in high TB-burden and resource-limited countries, and to facilitate integration of this evidence within practices and policies.
Specific :
- SO1: To collaborate with key stakeholders at local, national and international level, in order to ensure translation of scientific and operational evidence on TDAs into national policies and practices, scale-up plans at national level, and international paediatric TB guidelines, and to assess key determinants and processes for policy adoption;
- SO2: To implement a comprehensive TDA-based approach for childhood TB screening, diagnosis, and treatment decision-making, including shorter regimen for non-severe disease, in the context of a programmatic pilot, and using innovative digital data collection;
- SO3: To provide evidence on effectiveness, diagnostic accuracy, and cost-effectiveness of TDAs and identify adaptations required for specific sub-populations in order to inform policy change at a global and national level;
- SO4: To assess preferences, acceptability, and feasibility among end-users and beneficiaries, identify implementation challenges and provide tools for adapting and optimizing the implementation of TDAs in contexts with different health system organisation, resources and local epidemiology;
- SO5: To build capacity and continuously improve clinical practices of frontline HCWs for childhood TB through training, clinical mentoring, support supervision, and to design tools to facilitate translation of research results into improved clinical practices.
- Main Methods
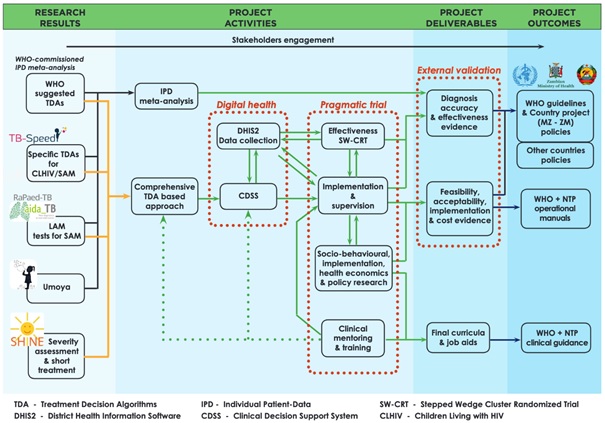
The concept of Decide-TB (figure 1 below) is to build on research results from several studies led by members of our consortium or to which we contributed: i) the WHO-commissioned Individual Patient Data (IPD) meta-analysis (2011-2012) on TDAs, ii) the Unitaid-funded TB-Speed diagnostic studies (2017-2022), iii) the UK Joint Global Health Trials-funded SHINE treatment trial (2016-2018), and iv) the EDCTP-funded RaPaed-TB and Umoya (2017- 2024) diagnostic studies. These results will be used for the design of a comprehensive TDA-based approach integrating TB screening, diagnosis, and treatment decision-making, and disease severity assessment for shorter treatment eligibility, for use at lower level of healthcare, and to be tested by NTPs in a programmatic pilot. We will develop a CDSS and strengthen district information systems (DHIS2) to collect individual data, which will contribute to monitoring and evaluation, clinical mentoring, and supervision by NTPs and to research in this proposal. The TDA-based approach will be tested in a hybrid effectiveness-implementation study based on a pragmatic stepped wedge cluster-randomized trial. In parallel, the diagnostic accuracy of different TDAs will be assessed through IPD meta-analysis of children with presumptive TB evaluated in recent prospective cohort studies. The pragmatic trial, the implementation research, and the IPD meta-analysis will contribute to thorough external validation of the WHO-suggested TDAs. Furthermore, engagement of key stakeholders and decision-makers throughout the project, following previously tested and effective strategies, will facilitate translation of the overall integrated TDA approach into clinical and implementation practices as well as policy at national and international levels.
Figure 1: Concept of Decide-TB
The workplan is structured into seven work packages (WP), each co-led by two consortium members, from sub-Saharan Africa and from Europe. The WPs will be integrated through continuous exchange between consortium members and interdisciplinarity collaboration (see figure 2).
WP1 (Project management and communication) co-led by the UBx and UNZA. The grant will be managed financially by UBx but Olivier Marcy (UBx) and Chishala Chabala (UNZA) will be jointly responsible for the coordination of the consortium and for the overall workplan. WP1 will include the organisation of the scientific, administrative, and financial aspects of the project. It will also include dissemination and communication activities, as well as the engagement of key stakeholders, starting from inception and continuing throughout the project.
WP2 (Pragmatic effectiveness trial) co-led by UBx (Olivier Marcy) and SU (Graeme Hoddinott). This WP will include the design, coordination, and analysis of a pragmatic cluster randomized trial, evaluating the deployment and prospective testing of TDA (implementation led by WP6) in Mozambique and Zambia. European and African clinical epidemiologists (Olivier Marcy, Celso Khosa (INS), Chishala Chabala, and James Seddon, SU & ICL) and social scientists (Joanna Orne-Gliemann, UBx and Graeme Hoddinott) involved in this WP will use a hybrid effectiveness-implementation approach and data collected in WP6 using WP5-initiated digital health tools, and mixed methods to provide scientific evidence on the effectiveness, feasibility and acceptability of TDAs implementation.
WP3 (Diagnostic accuracy) co-led by LMU (Laura Olbrich) and SU (Marieke van der Zalm). It will consist of an individual patient data (IPD) meta-analysis of children with presumptive TB evaluated in already completed, high quality, prospective cohort studies, funded by EDCTP. This WP will evaluate the diagnostic accuracy of the WHO-suggested TDA using available cohorts and will integrate closely with the TDA implementation and effectiveness assessment (WP2, 4, 6) and with policy development (WP7).
WP4 (Clinical practice) co-led by UNZA (Chishala Chabala) and IRD (Maryline Bonnet). It will contribute to practical integration of the TDA-based approach in local clinical practices, provide the clinical materials and standard operating procedures that can be used in WP5 to develop digital tools and in WP6 to train clinicians in the field for the deployment of the TDAs.
WP5 (Digital health), led by INS (Celso Khosa), with a strong contribution from the IT team in UBx. It will focus on strengthening national data collection systems for childhood TB (DHIS2), to support routine program monitoring (WP6), and a CDSS to support clinicians at PHC and DH in using the overall TDA-based approach.
WP6 (Implementation) co-led by the Zambia NTP (Patrick Lungu) and UBx (Joanna Orne-Gliemann). It will be responsible for deploying the integrated TDA-based approach at district-level through national systems, with the support of the other technical and scientific WPs. It will train HCWs, supervise and monitor implementation and will evaluate the implementation strategies every quarter, in partnership with WP2, within a rapid assessment and feedback approach, with adaptations and optimisations continuously implemented in real time.
WP7 (Modelling, health economics and policy) co-led by the UEM and USFD. Peter Dodd (USFD) and his team will undertake health economic analyses of TDA implementation. In addition, Regio Conrado (UEM) will evaluate how the TDA is integrated into policy at national and interventional levels.
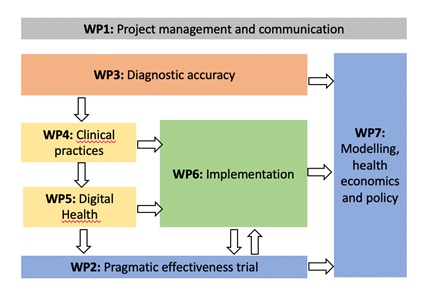
Figure 2: Decide-TB PERT diagram
[1] https://www.who.int/news-room/articles-detail/call-for-expressions-of-interest--generation-of-data-to-externally-validate-treatment-decision-algorithms-for-tuberculosis-in-children
